NanoFx®
Advanced Bone Marrow Stimulation System

What Is NanoFx?
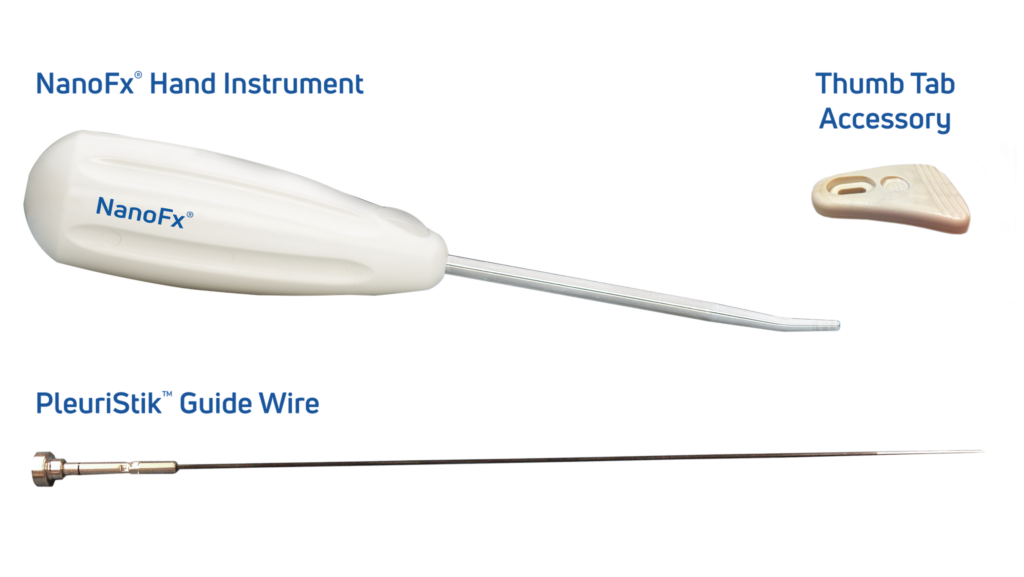
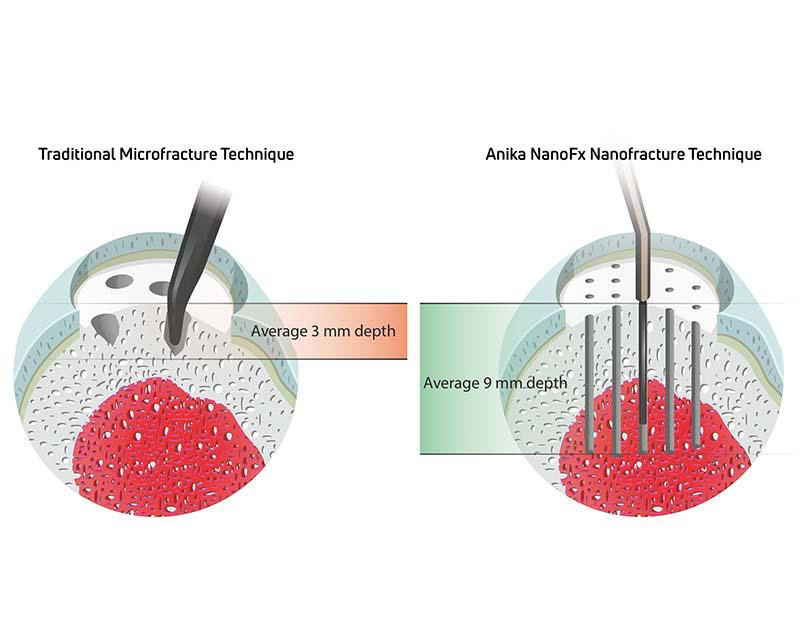
NanoFx® (Nanofracture®) is redefining standard microfracture procedures for the treatment of small, localized articular cartilage defects. Its 1mm diameter PleuriStik™ disrupts less surface area than a standard microfracture technique and was purposefully designed to reduce damage to the subchondral plate. Penetrating down to a 9 mm depth, NanoFx provides improved access to the targeted marrow cells, allowing for an enhanced healing environment three times deeper than standard microfracture awl techniques.
Used to improve the tissue repair response, such as cartilage lesions or rotator cuff tears, NanoFx provides significantly better results compared to traditional microfracture.1,2
Real Life Advantages
This approach to microfracture provides several advantages when compared to standard bone marrow stimulation procedures:
Smaller
The smaller 1mm diameter of the NanoFx Pleuristik causes less trauma to the subchondral bone surface and may provide a greater perforation density compared to the much larger 2.5mm microfracture awl.3
Deeper
Perforating down to 9mm versus a depth of 2mm improves access to the targeted marrow cells needed to initiate a healing response. Preclinical data demonstrates that the improvement in repair tissue quality and quantity was statistically significant due to deep versus shallow drilling.4
Better
Chondral repairs assessed after 12 months revealed that nanofracture provided better healing at the footprint over microfracture, with better cartilage architecture and greater type II collagen content achieved.1
Compared to traditional microfracture and k-wire procedures, NanoFx showed superior bone marrow access with multiple trabecular access channels extending 9mm into subchondral bone.5
The Science Behind NanoFx
Improved Access to Marrow Cells
The 9mm perforation depth provides deep cancellous bone perforation with improved access to targeted marrow cells.
More Holes
The NanoFx PleuriStick guide wire is only 1mm thick. This lets the surgeon place more holes in the defect area than you can with a microfracture awl, potentially increasing the amount of targeted marrow cells accessed.
Open Trabecular Channels
The NanoFx PleuriStick has a specific design that, as the guide wire is being removed, it clears the bone that was pushed down when the guide wire was inserted, allowing the trabecular channels to stay open.
Less Subchondral Bone Damage
The 1mm thick NanoFx PleuriStick disrupts less bone surface area than a standard microfracture technique, reducing damage to the subchondral bone plate.
Always Sharp
Unlike awls that can become dull over time, the tip of the PleuriStick guide wire is always sharp due to the fact that it is a single use instrument.
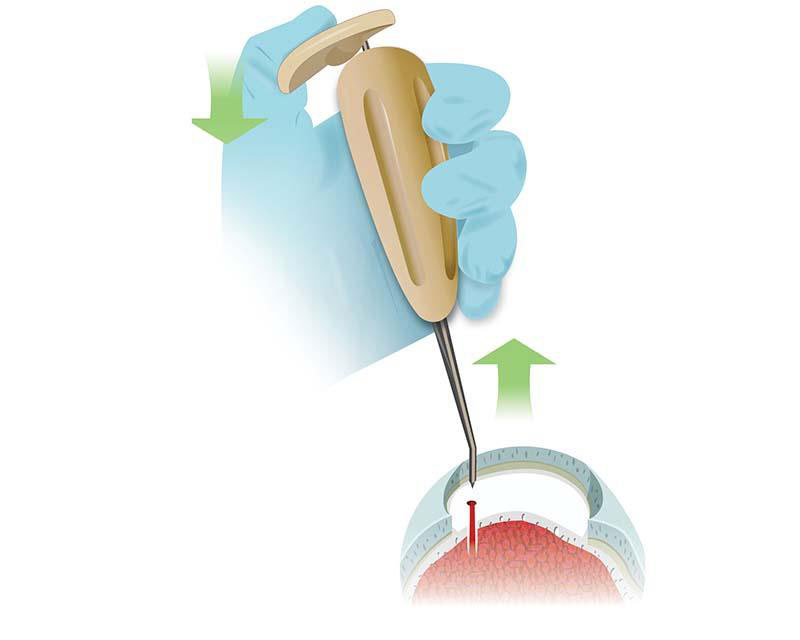
How It Works
NanoFx Microfracture System promotes cartilage repair by stimulating the body’s natural healing response through a minimally invasive technique:
Creates microfracture channels
in the subchondral bone using a precision-guided wire, allowing access to bone marrow
Releases mesenchymal stem cells (MSCs)
from the bone marrow into the defect site, initiating the repair process
Encourages formation of new cartilage tissue
which fills the defect with repair tissue resembling native hyaline cartilage
Evidence
When tested against an awl or generic k-wire, NanoFx produced thin, fragmented cancellous bone channels without rotational heat generation. It achieved deeper bone perforation and a higher number of open trabecular channels, optimizing marrow access and minimizing bone trauma.6
Bone marrow stimulation has long been a successful approach for cartilage repair, particularly in young, active patients with small defects. However, limitations of conventional microfracture, such as shallow penetration and channel clogging, led to the development of NanoFx, which creates 1mm wide, 9mm deep channels. This depth enables more consistent access to mesenchymal stem cells and enhances biological response.7,8,9
Drill-free bone perforations optimize trabecular bone venting and avoid channel closure from K-wire drilling caused by bone deposits that clog the trabecular tributaries. Studies have shown that deeper marrow access leads to an improved biological response and better tissue quality.4, 10
The sharp disposable needle tip provides better control during placement of the perforations and avoids slippage and damage to surrounding tissues.
The sharp disposable needle tip provides better control during placement of the perforations and avoids slippage and damage to surrounding tissues.
A Level I randomized controlled trial demonstrated that adding NanoFx nanofractures to the footprint during isolated supraspinatus tendon repair significantly improved healing outcomes.2 At 12-month follow-up, the re-tear rate was reduced by 50% compared to standard repair (19.4% vs. 42.4%, p = 0.038), with 94.4% of tendons successfully healed to bone in the NanoFx group versus 66.7% in controls (p = 0.014).1 This enhanced healing is attributed to deeper, more consistent marrow access and improved biological response at the tendon-bone interface.2
Select Publications & Clinical Data
Behrens et al., ICRS 2013
Key Takeaways
- NanoFx produced thin, fragmented cancellous bone channels without rotational heat generation
- It achieved deeper bone perforation and a higher number of open trabecular channels, optimizing marrow access and minimizing bone trauma
Chen H et al., J Orthop Res. 2011
Key Takeaways
- Deeper marrow access leads to an improved biological response and better tissue quality. NanoFx creates 9mm deep, 1mm wide channels, enhancing mesenchymal stem cell access
Chen H et al., J Orthop Res. 2009
Key Takeaways
- Drill-free bone perforations with NanoFx optimize trabecular bone venting and avoid channel closure from K-wire drilling caused by bone slurry deposits
Ruiz Ibán M et al., Knee Surg Sports Traumatol Arthrosc, 2020
Key Takeaways
- A Level I RCT showed that NanoFx nanofractures during supraspinatus tendon repair reduced re-tear rate by 50% (19.4% vs. 42.4%, p = 0.038) and improved healing (94.4% vs. 66.7%, p = 0.014
Resources
Product Information
Access comprehensive technical documentation and marketing materials
- Brochure
- Product Flyers
Instructions for Use
Complete product specifications and safety information
NanoFx is approved in the US and select markets outside of the United States for microfracture type procedures.
Anika products may not be available in all geographies. Product availability is subject to the regulatory clearances in individual markets. Please reach out to your local representative or Contact Us if you have questions about specific market approvals.
For complete product information, including indications, contraindications, warnings, and precautions, please refer to the Instructions for Use found here(opens in a new tab).
- Zedde P et al. Second Generation Needling Techniques for the Treatment of Chondral Defects in Animal Model. Joints 2017; 5:27–33 https://pmc.ncbi.nlm.nih.gov/articles/PMC5672857/pdf/10-1055-s-0037-1601412.pdf(opens in a new tab)
- Ibán M A R, et al. Footprint preparation with nanofractures in a supraspinatus repair cuts in half the re-tear rate at 1-year follow-up. A randomised controlled trial. Knee Surg Sports Traumatol Arthroscopy https://pmc.ncbi.nlm.nih.gov/articles/PMC8225541/pdf/167_2020_Article_6073.pdf(opens in a new tab)
- Benthien et al. Reviewing subchondral cartilage surgery: considerations for standardised and outcome predictable cartilage remodeling. International Orthopaedics (SICOT) 2013 https://pmc.ncbi.nlm.nih.gov/articles/PMC3824892/(opens in a new tab)
- Chen H et al. Depth of subchondral perforation influences the outcome of bone marrow stimulation cartilage repair. J Orthop Res. 2011 Aug;29(8):1178-84 https://onlinelibrary.wiley.com/doi/10.1002/jor.21386(opens in a new tab)
- Widuchowski W, Widuchowski J, Trsaska T. 2007. Articular cartilage defects: study of 25,124 knee arthroscopies. Knee 14:177–182 https://www.thekneejournal.com/article/S0968-0160(07)00027-0/abstract(opens in a new tab)
- Behrens et al., Bone Marrow Access in Cartilage Repair: Comparison of Microfracture, Nanofracture, K-wire, and Drill in the Adult Ovine Model., e-Poster: P87 Congress: ICRS 2013 https://nanofx.anika.com/wp-content/uploads/2021/10/Behrens-2013-Comparison-of-MicroFX-NanoFX-K-wire.pdf(opens in a new tab)
- Kreuz PC, Steinwachs MR, Erggelet C, Krause SJ, Konrad G, Uhl M, Südkamp N. Results after microfracture of full-thickness chondral defects in different compartments in the knee. Osteoarthritis Cartilage. 2006 Nov;14(11):1119-25. https://www.oarsijournal.com/action/showPdf?pii=S1063-4584%2806%2900150-6(opens in a new tab)
- Mithoefer K, Williams RJ 3rd, Warren RF, Potter HG, Spock CR, Jones EC, Wickiewicz TL, Marx RG. The microfracture technique for the treatment of articular cartilage lesions in tthe knee. A prospective cohort study. J Bone Joint Surg Am. 2005 Sep;87(9):1911-20 https://journals.lww.com/jbjsjournal/abstract/2005/09000/the_microfracture_technique_for_the_treatment_of.2.aspx(opens in a new tab)
- Steadman JR, Briggs KK, Rodrigo JJ, Kocher MS, Gill TJ, Rodkey WG. Outcomes of microfracture for traumatic chondral defects of the knee: average 11-year follow-up. Arthroscopy. 2003 May-Jun;19(5):477-84. https://www.arthroscopyjournal.org/article/S0749-8063(03)00124-5/abstract(opens in a new tab)
- Fortier LA, Cole BJ, McIlwraith CW. Science and animal models of marrow stimulation for cartilage repair. J Knee Surg 2012;25:3-8. https://pubmed.ncbi.nlm.nih.gov/22624241/(opens in a new tab)
- Chen H, Sun J, Hoemann CD, et al. Drilling and microfracture lead to different bone structure and necrosis during bone-marrow stimulation for cartilage repair. J Orthop Res. 2009 Nov;27(11):1432-8. https://onlinelibrary.wiley.com/doi/epdf/10.1002/jor.20905(opens in a new tab)